Introduction
Human dentition presents a variety of anatomical and morphological variations. The anatomy of the root canal system dictates the conditions under which root canal therapy is carried out and can directly affect its prognosis1. One of the most important abnormalities in tooth morphology is taurodontism. This abnormality is a developmental disturbance of a tooth that lacks constriction at the level of the cementoenamel junction (CEJ) and is characterized by vertically elongated pulp chambers, apical displacement of the pulpal floor, and bifurcation or trifurcation of the roots2 (Fig 1). Taurodontism, although not common, is an important occurrence that may influence dental management of patients.
External morphology was first used to describe those teeth that had apically displaced furcation areas. It was first described by Gorjanovic´-Kramberger K.3; although the earliest example of taurodontism is that of the Krapina Neanderthal race, 70,000 years old anthropological specimen4. However, the term taurodontism was first introduced by Sir Arthur Keith5 to describe molar teeth resembling those of ungulates, particularly bulls. So, the term taurodontism comes from the Latin term 'tauros', which means 'bull' and the Greek term 'odus', which means 'tooth' or 'bull tooth'5.
 | Fig 1: Taurodontism
 |
Incidence
Witkop CJ6 suggested that taurodontism was found more often in people in which teeth were used as tools, as more advantageous than cynodontism in people with heavy masticatory habits. It has also been seen in Eskimos, Europeans, African Americans, and in white Americans7. However, Sciulli PW8 found no evidence of taurodontism in prehistoric American Indians, people who must have also used their teeth extensively.
Pindborg JJ9 stated that the prevalence of taurodontism in modern man is less than 0.1%. However, Blumberg JE et al.10 found it in about 2.5% of cases. Keene HJ11 reported hypo taurodontism in 2.8% of cases and mesotaurodontism in 0.4% cases. Further, Shifman A and Chanannel I12 showed hypo taurodontism in 5.2% of cases, mesiotaurodontism in 1.0% and hyper taurodontism in 0.7%. So, they suggested that taurodontism is not rare in modern man as previously thought, infact hypotaurodontism is just variation of normal, but hypertaurodontism is yet a rare entity.
The teeth involved are mostly molars-sometimes only a single tooth and other times several molars in the same quadrant. Sert S. and Bayrili G.13 reported a patient that had six taurodont molar teeth, 4 maxillary and two mandibular molars. Similarly, Shifman A and Buchner A14 reported that in one case, eight teeth were taurodonts. The mandibular second molar is the most prone, being involved in two third of all the cases found 12, 14. It is reported that the degree of taurodontism increases from the first to the third molar 2,15. Also, reported that taurodontism is occasionally observed in mandibular and maxillary premolars, and even mandibular canines and incisors15, 16.
Taurodontism may affect the deciduous or permanent dentition2,17,18,19. The condition may be unilateral or bilateral and in any combination of teeth or quadrants20. Shifman A and Buchner A14 also reported that the majority of the affected teeth occurred singly. However, Laatikainen T and Ranta R21 found that taurodontism was symmetrical in 91% of the affected molar pairs.
The gender distribution of the patients with taurodontism showed no statistically significant difference21 except for a higher prevalence amongst females in a Chinese population17.
Etiology
The etiology of taurodontism is unclear. It is thought to be caused by the failure of Hertwig's epithelial sheath diaphragm to invaginate at the proper horizontal level, resulting in a tooth with short roots, elongated body, an enlarged pulp, and normal dentin22. Interference in the epitheliomesenchymatose induction has also been proposed as a possible aetiology23.
Previously, taurodontism was related to various syndromes such as Down's and Klinefelter's24. So suggested that taurodontism may be genetically transmitted25, 26. Varrela J and Alvesalo L27 supported the concept that the prevalence of taurodontism increases as the number of X chromosomes increases and also indicate that expression of the trait and the number of X chromosomes may be positively correlated. They have further suggested that the X chromosome gene(s) influencing development of enamel may also be involved in the development of taurodontism.
Except genetic transmission, other external factors can also damage developing dental structures in children and adolescents as infection (osteomyelitis)28, disrupted developmental homeostasis29, high-dose chemotherapy30, and a history of bone marrow transplantation31.
But now a days, taurodontism especially hypotaurodontism is considered as an anatomic variance that could occur in a normal population12.
Classification
The common problem that arises in taurodontism is that there are differences of opinion regarding how much displacement and how much morphologic change constitutes taurodontism. Another problem complicating accurate assessment of the incidence of taurodontism is the inclusion of premolars or anteriors by many investigators32,23, whereas others have questioned this inclusion33.
Shaw JCM gave first classification ever done for taurodonts in the year 1928, according to its severity34: normal tooth- cynodont; least pronounced-hypotaurodontism: moderate enlargement of the pulp chamber at the expense of the roots; moderate - mesotaurodontism: pulp is quite large and the roots short but still separate; and most severe- hypertaurodontism: prismatic or cylindrical forms where the pulp chamber nearly reaches the apex and then breaks up (Fig 2). This classification is usually preferred but it is not an objective analysis.
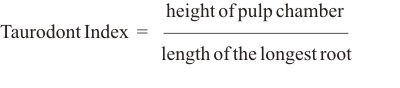
Keene HJ11 in 1966 gave the taurodont index in order to classify the degree of taurodontism as ratio of height of pulp chamber to the length of the longest root.
 | Fig 2: Classification Of Taurodontism
|
According to this index, value of
0 - 24% is cynodont,
25- 49.9% is hypotaurodont,
50- 74.9% is mesotaurodont
and 75- 100% is hypertaurodont.
The major drawback of this index is that it makes use of landmarks in biological structure which are liable to change with time due to formation of reparative dentin.
Another method was discussed by Blumberg et al.10 in 1971. Though his landmarks were relatively stable, but the formula was quite cumbersome for regular clinical use.
So, Feichtinger C & Rossiwall B.34 further on the basis of the work of earlier authors, gave an easier method and stated that if the distance from the furcation of the roots to the cementoenamel junction was greater than the occlusal cervical distance, taurodontism is present.
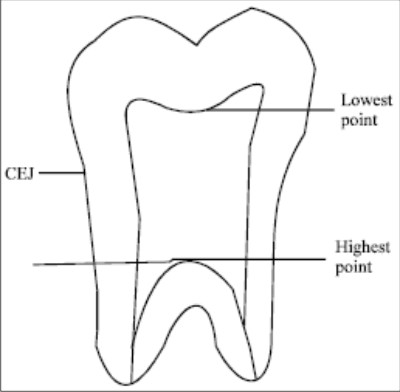
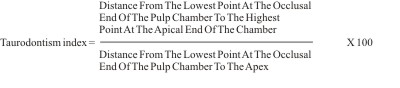
Further, Shifman A and Chanannel I12 in 1978 also included an index to calculate the degree of taurodontism as shown radiographically. It was based on the relative amount of apical displacement of the pulp chamber floor. As per their index, taurodontism is present if the distance from the lowest point at the occlusal end of the pulp chamber (A) to the highest point at the apical end of the chamber (B) divided by the distance (b) from A to the apex is 0.2 or greater; and if the distance from the highest point at the apical end of the chamber to the cementoenamel junction (CEJ) is greater than 2.5 mm.
 |
|
Degree of taurodontism was determined to be: hypotaurodontism if TI is 20-30%, mesotaurodontism if TI is 30-40% and hyper taurodontism if TI equals 40-75%12.
This index has overcome many disadvantages of previous methods, however in few cases this formula fails, as in teeth that subjectively appeared to be taurodonts but did not meet the above criteria33 due to strange pulp configuration.
In addition to all these methods, Tulensalo T. et al.36 examined a simple method of assessing taurodontism using orthopantomograms (OPG) by measuring the distance between the baseline (connecting the mesial and distal points of the CEJ) and the highest point of the floor of the pulp chamber. They concluded that this technique is reliable in epidemiologic investigations for assessing taurodontism in a developing dentition.
Clinical and radiographic features
A taurodontic tooth has certain anatomic characteristics. First, the cervical constriction is less marked than the normal tooth form. Further, the tooth must have an apically displaced furcation and short roots. However, clinically the taurodont appears as a normal tooth because body and roots of a taurodont lie below the alveolar margin.
Radiographically, involved teeth are frequently found to be rectangular in overall shape rather than tapering toward the roots. The pulp chamber is extremely large with a much greater apico-occlusal height than normal. In addition, the pulp lacks the usual constriction at the cervical region of the teeth and the roots are exceedingly short. The bifurcation or trifurcation may be only a few millimeter above the apices of the roots.
Diagnosis
The above described external features have been primarily used for the diagnosis of taurodontism. However, it should be noted that gross external characteristics are not sufficient to generate diagnosis15. Further, clinical crowns of these teeth have near to normal characteristics; therefore, taurodontism may be diagnosed only radiologically either from IOPA or OPG.
Syndromes
Taurodontism appears mostly as an isolated anomaly; but it has also been associated with several syndromes like Down syndrome, Klinefelter's syndrome, trichodento-osseous syndrome, and others37-42. Many of these disorders have oral manifestations, which can be detected on dental radiographs as alterations in the morphology or chemical composition of the teeth.. So, dentist being familiar with taurodontism may disclose systemic problems that would otherwise remain undetected6. Several patients with taurodontism associated with some other recognizable dental anomaly are seen. In these cases, there is no reason to suspect that taurodontism and the other anomaly were linked.
Clinical Significance
The presentation of taurodont forms complicates nonsurgical, endodontic procedures because of the impact of the morphology on location of orifices and instrumentation and obturation43. Although there is a characteristic radiographic picture, the pretreatment films provide little information about the root canal system23. Finally, the results of pulp testing contribute little information about the effect of a large pulp chamber on tooth sensitivity43.
There are different views regarding access cavity design and preparation: Shifman A & Buchner A14 argued that access to the root canal orifices can easily obtained as the floor of the pulp chamber cannot affected by the formation of reactionary dentine as in normal teeth. In contrast, Durr et al.44 suggested that morphology could hamper the location of the orifices, thus creating difficulty in instrumentation and filling. It also shows wide variation in the size and shape of the pulp chamber, varying degrees of obliteration and canal configuration, apically positioned canal orifices, and the potential for additional root canal systems.
A complicated root canal treatment has been reported for a mandibular taurodont tooth with five canals, only three of which could be instrumented to the apex45. Therefore, careful exploration of the grooves between all orifices is recommended to reveal additional orifices and canals. Further use of magnification43 is helpful in easy location of the canal orifices.
Because the pulp of a taurodont is usually voluminous, in order to ensure complete removal of the necrotic pulp, 2.5% sodium hypochlorite has been suggested initially as an irrigant to digest pulp tissue46. Moreover, as adequate instrumentation of the irregular root canal system cannot be anticipated47, suggested that additional efforts should be made by irrigating the canals with 2.5% sodium hypochlorite in order to dissolve as much necrotic material as possible. Application of final ultrasonic irrigation may ensure that no pulp tissue remains46.
Finally, it should be noted that in cases of hypertaurodont (where the pulp chamber nearly reaches the apex and then breaks up into two or four channels) vital pulpotomy instead of routine pulpectomy may be considered as the treatment of choice2, 14.
Because of the complexity of the root canal anatomy and the proximity of the buccal orifices, complete filling of the root canal system in taurodontism is challenging. A modified filling technique has been proposed, which consists of combined lateral compaction in the apical region with vertical compaction of the elongated pulp chamber, using the system B device (EIE / Analytic Technology, San Diego, CA, USA)43.
About the surgical part, extraction of a taurodont tooth is usually complicated because of a dilated apical third24. In contrast, it has also been hypothesized that because of its large body, little surface area of a taurodont tooth is embedded in the alveolus. This feature would make extraction less dif?cult44.
For the prosthetic treatment of a taurodont tooth, it has been recommended that post-placement be avoided for tooth reconstruction43. Further as less surface area of the tooth is embedded in the alveolus, a taurodont tooth may not have as much stability as a cynodont when used as an abutment for either prosthetic or orthodontic purposes44.
From a periodontal standpoint, taurodont teeth may, in specific cases, offer favorable prognosis. Where periodontal pocketing or gingival recession occurs, the chances of furcation involvement are considerably less than those in normal teeth because taurodont teeth have to demonstrate significant periodontal destruction before furcation involvement occurs2, 14.
Conclusion
It can be seen that taurodontism has received insufficient attention from clinicians. Special attention is required to indentify the anomaly. In performing root canal treatment on these teeth, one should appreciate the complexity of the root canal system. Careful exploration of the grooves between all orifices, particularly with magnification; ultrasonic irrigation; and a modified filling technique are recommended. Care should also be exercised during extractions and post endodontic rehabilitation. Finally although taurodontism is a dental rarity, this unusual radicular form should be considered during planning the treatment.
References
1. Slowey RR. Root canal anatomy: road map to successful endodontics. Dent Clin North Am 1979; 23: 555-73.
2. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral & Maxillofacial Pathology, 5th edn. Philadelphia: W.B. Saunders. 2002
3. Gorjanovic Kramberger K. Über prismatische molarwurzein rezenter und diluvialer menschen. Anatomischer Anzeiger 1908; 32: 401-13.
4. Barker BCW. Taurodontism: the incidence and possible significance of the trait. Aust Dent J 1976; 21: 272-6.
5. Keith A. Problems relating to the teeth of the earlier forms of prehistoric man. J Royal Soc Med 1913; 6: 103-24.
6. Witkop CJ. Clinical aspects of dental anomalies Int Dent J 1976; 26: 378-90.
7. Mjör IA. The structure of taurodont teeth. J Dent Child 1972; 39: 459-63.
8. Sciulli P W. A descriptive and comparative study of the deciduous dentition of prehistoric Ohio Valley Amerindians. Am J Phy Anthropol 1977; 47: 71-80.
9. Pindborg JJ. Pathology of the dental hard tissues. Munksgaard, Copenhagen 1970, p.44.
10. Blumberg JE, Hylander WL., Goepp RA. Taurodontism, a biometric study. Am J Phy Anthropol 1971; 34: 243-256.
11. Keene HJ. A morphological and biometric study of taurodontism in a contemporary population. Am J Phys Anthropol. 1966; 25: 208-209.
12. Shifman A, Chanannel I. Prevalence of taurodontism found in radiographic dental examination of 1200 young adult Israeli patients. Com Dent Oral Epidemiol 1978; 6: 200-3.
13. Sert S, Bayrili G. Taurodontism in six molars: a case report. J Endod 2004; 30: 601-2.
14. Shifman A, Buchner A. Taurodontism: Report of sixteen cases in Israel. Oral Surg Oral Med Oral Pathol 1976; 41: 400-405.
15. Mena CA Taurodontism. Oral Surg Oral Med Oral Pathol 1971; 32: 812-23.
16. Osborn JW. Dental Anatomy and Embryology. Oxford: Blackwell scienti?c publications. 1981.
17. MacDonald-Jankowski DS, Li TT. Taurodontism in a young adult Chinese population. Dent MaxilloFac Radiol 1993; 22: 140-4.
18. Goaz PW, White SC. Oral Radiology (Principles and Interpretation), 3rd edn. Louis, USA: Mosby. 1994
19. Rao A, Arathi R Taurodontism of deciduous and permanent molars: report of two cases. J Ind Soc Pedo Prev Dent 2006; 24: 42-4.
20. White SC, Pharoah MJ. Oral Radiology. Principles and Interpretation, 5th edn. St.Louis, USA: Mosby 2004.
21. Laatikainen T, Ranta R. Taurodontism in twins with cleft lip and / or palate. European J Oral Sci 1996; 104: 82-6.
22. Hamner J E, Witkop CJ, Metro PS. Taurodontism. Report of a case. Oral Surg Oral Med Oral Pathol 1964; 18: 409-18.
23. Llamas R, Jimenez-Planas A. Taurodontism in premolars. Oral Surg Oral Med Oral Pathol 1993; 75: 501-5.
24. Yeh SC, Hsu TY. Endodontic treatment in taurodontism with Klinefelter's syndrome: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 88: 612-5.
25. Goldstein E, Gottlieb MA. Taurodontism: familial tendencies demonstrated in eleven of fourteen case reports. Oral Surg Oral Med Oral Pathol 1973; 36: 131-44.
26. Witkop CJ. Manifestation of genetic disease in the human pulp. Oral Surg Oral Med Oral Pathol 1971; 32: 278-316.
27. Varrela J, Alvesalo L. Taurodontism in females with extra X chromosomes. J Craniofac Genet Dev Biol 1989; 9: 129-33.
28. Reichart P, Quast U. Mandibular infection as a possible aetiological factor in taurodontism. J Dent 1975; 3: 198-202.
29. Witkop CJ Jr, Keenan KM, Cervenka J, Jaspers MT. Taurodontism: ananomaly of teeth re?ecting disruptive developmental homeostasis. Am J Med Genetics 1988; 4: 85-97.
30. Greenberg MS, Glick M Burket's Oral Medicine- Diagnosis and Treatment, 10 th edn. Hamilton, ON, Canada: BC Decker 2003
31. Vaughan M D, Rowland CC, Tong X Dental abnormalities in children preparing for pediatric bone marrow transplantation. Bone Marrow Transplant 2005; 36: 863-6.
32. Madeira MC, Leite HF, Niccoli Filho WD, Simoes S. Prevalence of taurodontism in premolars. Oral Surg, Oral Med Oral Pathol 1986; 61: 158-62.
33. Ruprecht A, Batniji S, el-Neweihi E. The incidence of taurodontism in dental patients. Oral Surg, Oral Med Oral Pathol 1987; 63: 743-7.
34. Shaw J C M. Taurodont teeth in South African Races. J Anat 1928; 62: 476-99.
35. Feichtinger C, Rossiwall B. Taurodontism in human sex chromosome aneuploidy. Arch Oral Biol 1977; 22:327-329.
36. Tulensalo T, Ranta R, Kataja M. Reliability inestimatIng taurodontism of permanent molars from orthopantomograms. Comm Dent Oral Epidemiol 1989; 17: 258-62.
37. Chichon JC, Pack RS. Taurodontism: review of literature and report of case. J Am Dent Assoc 1985; 111: 453-5.
38. Jaspers MT, Witkop CJ Jr. Taurodontism, an isolated trait associated with syndromes and X-chromosomal aneuploidy. Am J Hum Genet 1980; 32; 396-413.
39. Alfred MJ, Crawford PJ. Variable expression in amelogenesis imperfecta with taurodontism. J Oral Pathol 1988; 17:327-33.
40. Ogden GR. Taurodontism in dermatologic disease. Int J Dermatol 1988; 27: 360-4.
41. Bell J, Civil CR, Townsend GC, Brown RH. The prevalence of taurodontism in Down's syndrome. J Ment Defic Res 1989; 33: 467-76.
42. Lichtenstein JR, Warson R, Jorgenson R, Dorst JP, Mc Kusick VA. The trichodento-osseous (TDO) syndrome. Am J Hum Genet 1972; 24: 569-82.
43. Tsesis I, Shifman A, Kaufman AY. Taurodontism: an endodontic challenge. Report of a case. J Endod 2003; 29: 353-5.
44. Durr DP, Campos CA, Ayers CS Clinical signi?cance of taurodontism. J Am Dent Assoc 1980; 100: 378-81.
45. Hayashi Y. Endodontic treatment in taurodontism. J Endod 1994; 20: 357-8.
46. Prakash R, Vishnu C, Suma B, Velmurugan N, Kandaswamy D (2005) Endodontic management of taurodontic teeth. Indian J Dent Res 2005; 16: 177-81.
47. Widerman FH, Serene TP (1971) Endodontic therapy involving a taurodontic tooth. Oral Surg, Oral Med and Oral Path 1971; 32: 618-20. |